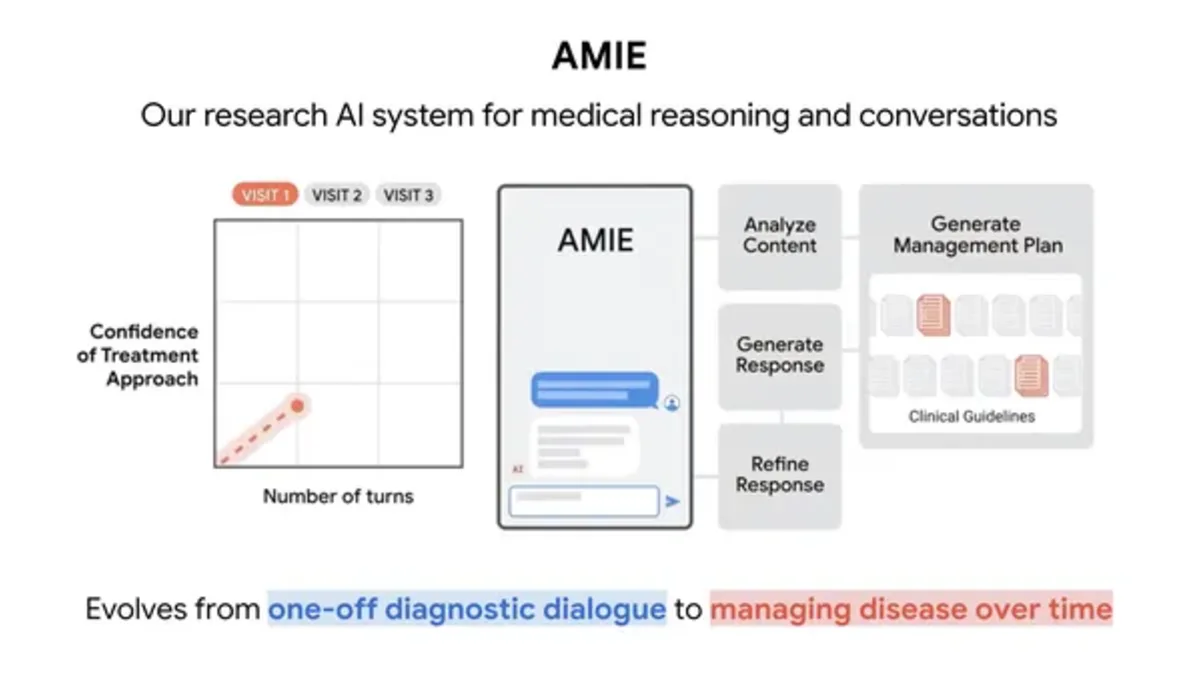
Medical AI is moving from simple symptom explanation toward more complex conversations about ongoing care. That shift is important because managing a health condition is rarely a single question. Patients need to understand tradeoffs, habits, risks, medication routines, warning signs, and when to return to a clinician. A useful assistant has to keep context without pretending to be a doctor.
Google's AMIE research is part of that next phase. A medical conversation system that can handle disease-management scenarios is different from a general chatbot that answers health questions. It has to reason across patient goals, safety limits, follow-up needs, and clinical uncertainty. It also has to communicate in a way that a patient can understand without flattening important nuance.
The promise is not hard to see. Health systems are overloaded, chronic conditions require steady support, and patients often leave appointments with questions they remember later. A carefully designed AI assistant could help people prepare for visits, understand care plans, track concerns, and ask better questions. The danger is equally clear: a model that oversteps can create false reassurance or unnecessary alarm.
Google reported that research in Nature showed AMIE matching primary care physicians in complex disease-management conversations in the studied setting. That is a research milestone, not a reason to treat AI as a replacement for clinical care. The setting, evaluation design, and guardrails matter.
The work connects with the broader health-data pressure we covered in wearable health data overload in clinics. Patients and devices are generating more information than care teams can easily process. Specialized assistants may help organize that information, but they must not create another stream of unverified recommendations for clinicians to clean up.
Specialization is the key. A medical AI system should not behave like a general productivity assistant with a hospital theme. It needs domain evaluation, safety behaviors, escalation rules, careful language, and transparency about what it knows. It should also understand when a question requires urgent human attention. In health, a good refusal or escalation can be just as valuable as a direct answer.
There is also a deployment problem. Research performance does not automatically translate to real clinics. Real patients have incomplete histories, multiple conditions, language barriers, insurance constraints, and emotional stress. Doctors work with time pressure, liability, records systems, and local protocols. Any AMIE-like system would need to fit into that messy environment before it can be trusted at scale.
Google's research shows why specialized medical AI is becoming more credible. It also shows why the bar should stay high. The best future for systems like AMIE is not replacing care teams. It is giving patients clearer support between visits and helping clinicians focus on judgment rather than repetitive explanation. That is a valuable goal, but only if safety and accountability grow with the capability.
The next phase should be judged by deployment evidence, not only research comparisons. Clinicians will want to know how the assistant handles edge cases, missing data, emergency cues, and patient misunderstanding. Patients will want language that feels clear without becoming overconfident. AMIE's promise is real, but healthcare earns trust one controlled rollout at a time.

